
The benefits of routine screening for developmental dysplasia of the hip
Dr Sue Charlton’s PhD research has been underpinned by decades of work with children in regional and rural South Australia. Here she outlines the need for a routine screening ultrasound to identify infants at risk of developmental dysplasia of the hip.
Continuously working in a solo paediatric practice in one regional centre in South Australia over the past forty-nine years has led to a strong interest in the retention of allied health workers in rural and regional areas.
For me, it has been a great privilege to work with families over this length of time, in several instances three generations of the same family.
Living in the community, you are continually aware of the successes and failures of the work done.
Continuity of care offers great opportunities to experience the long-term effects of treatment and management.
It expounds the need to remain current and aware of the latest developments in treating and managing paediatric conditions.
It is also a constant reminder of how physiotherapy has changed over a lifetime of living in the same environment as your patients.
Your successes and failures live with you.
It is an extreme privilege to become an integral part of many families and to share their good and hard times as our children grow up.
Developmental dysplasia of the hip
Working with teenagers experiencing gait difficulties and joint range limitations following late diagnosis of their dysplastic hips has been monumental in my research interest.
Being confronted by a mother wondering why her baby is late walking or has an uneven gait, knowing that an X-ray will likely reveal a dislocated hip, gives you an unpleasant vision of what lies ahead.
There will be extensive treatment in their early years, with splintage and surgery.
Surgical possibilities have developed but these children often become sensitive about their gait and suffer restriction of movement, with early arthritis.
Very early joint replacement is a real possibility.
Reliable and measurable hip status in the early weeks after birth should be available to all babies.
Neonatal instability of the hip
It is well recognised that the timely diagnosis of developmental dysplasia of the hip is crucial to lifetime hip development.
What is less well recognised is that an assessment of neonatal instability of the hip can be a predictor of developmental dysplasia of the hip.
Early accurate measurement of neonatal instability of the hip is not only a predictor of later hip development, it also offers the opportunity to provide early education about hip development and optimal ways of influencing this within the first few months of infant life.
This must be an important part of the paediatric physiotherapist’s role as both a preventer of disability and an educator in optimal infant management.
Infant management
There have been significant changes in infant management over the past 20 years, with safe-sleeping techniques and an increased need for baby wrapping, which have influenced baby development.
The difficulty of maintaining a midline head position in a newborn infant, when muscle tone does not support head control against gravity, leads to a tendency for an asymmetrical head position, causing flattening of the head on the preferred side.
This then leads to constant return to that side where the head sits comfortably.
Asymmetrical posturing is projected onto the trunk and legs.
We see trunk incurvature away from the preferred side and increased adduction of the crown-side leg and abduction of the chin-side leg.
This asymmetry places the adducted leg at great risk of poor development, as the femoral head on that side is not directed into the base of the developing acetabulum, often sitting out a small distance.
Firm containment of the femoral head within the developing acetabulum, where the three seed ossification centres of the pelvis meet, is conducive to the formation of a nicely fitting hip socket.
Supine sleeping is not a customary position for many animals.
Normally they sleep with the bony protection of the spine, posterior cranium and pelvis to the world and cover their more vulnerable abdominal wall and genitalia.
Perhaps for this reason, newborn babies do not settle confidently when sleeping supine.
Poor settling has led to firm wrapping or swaddling of infants to encourage a feeling of security.
The extended, adducted positioning of the legs draws the femoral head away from its centralised position in the base of the developing acetabulum.
All newborn infants have some degree of instability in their hips in the early weeks after birth.

Dr Sue Charlton's research focuses on developmental problems in infancy, such as developmental dysplasia of the hip, and the impact of regionality.
Early anterior dynamic ultrasound (eADUS) provides accurate and measurable assessment of the stability of the infant hip joint, while Graf ultrasound examination, shown to be variable prior to six weeks of age (Cundy 2004), gives accurate and measurable information about the morphology of the hip joint.
It is important to differentiate between what is examined with eADUS and with the Graf ultrasound.
We must stop comparing these two examinations and concentrate on comparing results from early clinical assessment of infant hips and eADUS, because these are the two assessments we are currently evaluating.
Each of these examinations has an established standard of measurement that has been accepted in international studies (Andersson 1995).
Criticism has been levelled at the reliability of clinical assessment of infant hips in regional South Australia, where reliability is deemed to be experience-dependent (Azzopardi et al 2011).
Studies show that at least 100 examinations are necessary to develop the ability to reliably make a clinical assessment of infant hips (Goss 2002).
Studies have stated that clinical assessment is most reliably made by paediatric orthopaedic specialists (Paton 2005).
Other studies have shown that both experienced physiotherapists and child health nurses can achieve similarly reliable results (Bloomfield et al 2003).
The pertinent word here is ‘experienced’.
Research
My PhD study (Charlton 2019) examined the use and acceptance of eADUS in the assessment of infant hips in the first two weeks after birth.
A study in two regional centres in South Australia sought to uncover any differences between the two centres.
As often happens in PhD studies, unexpected and wider differences than had been anticipated were discovered.
This led to a deeper examination of health expectations and understanding in regional South Australia.
When it became impossible to continue the screening through the radiology department due to fears of criticism of overservicing, it was decided to offer a hip screening service at the physiotherapy practice for those parents wishing to see their infant’s hips on ultrasound.
A sonographer was employed, with parents invited to attend the screening clinic in the first two weeks after the birth of their baby.
Many physiotherapy practices use ultrasound in the management of musculoskeletal problems or as a biofeedback tool.
We use a portable, battery-powered ultrasound that can store images, which can be transmitted to an orthopaedic specialist if further examination is warranted.
Parents can see the infant hip and understand the development of the joint.
Advice can be given about optimum wrapping and management of the hip, with encouragement to commence tummy time during supervised wakeful periods.
The measurement standards outlined by Andersson (1995) have been adopted. In combination with early advice about hip care, parents of infants with greater than four millimetres of movement on first examination are advised to discuss further management with their family doctor.
A further scan is advised for these infants and may be either a further ADUS or a Graf ultrasound examination.
Those with greater than five millimetres movement on eADUS are discussed with the family doctor and referred to an orthopaedic specialist for follow-up.
Through our study we have discovered two infants with dislocated hips that were not noted on clinical assessment because they were not able to be relocated in the acetabulum on initial clinical assessment.
For these families, the early diagnosis has meant earlier reduction and splinting of the hip during a very important period of normal hip and milestone development.
We have found parents to be very enthusiastic about the eADUS, appreciating and understanding more about infant hip development.
Surprisingly, many parents subsequently report becoming aware of families impacted by hip problems after late diagnosis.
Most interestingly, we have seen that family history is as strong a predictor of problems as breech at term.
In fact, breech at term has been shown to be protective against late diagnosis because of the strong recommendations for early follow-up (Azzopardi et al 2011).
Surely this is an indication for eADUS of all infant hips.
It could occur in maternity units, with small, portable ultrasound machines, and should be a recommendation from physiotherapists.
In our studies we have used a mix of three different sonographers and three different physiotherapists and results have remained similar with different operators.
It has been our process for the physiotherapist to make a preliminary clinical assessment of the amount of movement felt on the standard clinical test.
Following the therapist’s estimation, a measurement is made on the eADUS scan.
Interesting improvement over time is seen in the accuracy of the therapist’s clinical assessment.
Recently we were faced with an eight-week-old infant who had not taken part in the early screening program.
Her hips were stated as clinically normal with no clunk or obvious displacement at birth.
The child health nurse noted asymmetrical leg posture on a home visit.
After the family doctor was consulted, a Graf ultrasound was ordered.
She was found to have a fully dislocated left hip, with the femoral head sitting posterior to the joint, unable to be seen in the joint at all.
The maternal grandmother had severe hip problems in her early 50s but was loath to have a hip replacement because of her age.
She reported that her hip became stiff with long car travel, clunking in and out of position on walking after a long drive.
This indeed constitutes family history and should indicate the need for close follow-up of any babies in this family to prevent such things in future generations.
As physiotherapists, we should be advocating for eADUS to be part of the neonatal assessment in maternity wards or in the first two weeks after birth, like the hearing tests that are already performed soon after birth.
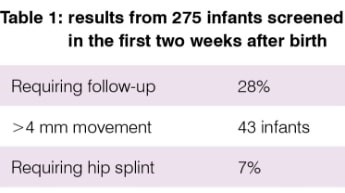
In our current study of 275 infants in the first two weeks after birth, we have examined infants born since April 2019 (Table 1).
The percentage requiring follow-up is skewed by the clinical guidelines requiring Graf ultrasound for all breech babies.
We found that only 17 per cent of breech babies had greater than 3.5 millimetres of movement.
Our figures are not a view of all babies born in this period.
It is likely that they are infants of parents who have been aware of previous studies conducted in Mount Gambier, infants with doubtful clinical assessments or infants who are are deemed to be at risk of hip problems, as they may be more likely to be recommended to attend the screening days.
Country word of mouth is a strong referrer too.
>> Sue Charlton AM, MACP is an APA Paediatric Physiotherapist in regional South Australia. She holds adjunct status with Flinders University and the University of South Australia and has studied, published and presented on developmental problems in infancy. She recently completed her PhD studies at Flinders University, where she studied the impact of regionality on families with infants who have developmental problems such as developmental dysplasia of the hip.
- References
. Cundy PR, J. Longitudinal study of neonatal hip ultrasound. Adelaide: Women's and Children's Hospital; 2004.
2. Andersson JE. Neonatal hip instability: normal values for physiological movement of the femoral head determined by an anterior-dynamic ultrasound method. J Pediatr Orthop. 1995;15(6):736-40.
3. Azzopardi T, Van Essen P, Cundy PJ, Tucker G, Chan A. Late diagnosis of developmental dysplasia of the hip: an analysis of risk factors. J Pediatr Orthop B. 2011;20(1):1-7.
4. Goss P. Successful screening for neonatal hip instability in Australia. Journal of Paediatric and Child Health. 2002;38(5):469 - 74.
5. Paton R. Screening for hip abnormality in the neonate. Early Hum Dev. 2005;81(10):803-6.
6. Bloomfield LR, C. Townsend, J. Wolke, D. Quist- Therson, E. The quality of routine examinations of the newborn performed by the midwives and SHOs: an evaluation using video recordings. JMed Screen. 2003;10(4):176-80.
7. Charlton S. Early dynamic ultrasound in the assessmentand management of neonatal instability of the hip: An intervention through health literacies to transform rural and regional health [Research]. Flinders University (online): Flinders university; 2019.
© Copyright 2024 by Australian Physiotherapy Association. All rights reserved.





{kind=link}