
High-value care following ACLR
Scott Wilson details the application of recommendations based on the best available practice guidelines in the case of a female adolescent presenting nine months after anterior cruciate ligament reconstruction.
The annual incidence of anterior cruciate ligament reconstruction (ACLR) in Australia has risen 43 per cent from 2000 to 2015 and by 74 per cent among those under the age of 25 (Zbrojkiewicz et al 2018).
Zbrojkiewicz et al (2018) also state that the incidence of ACLR is increasing most rapidly among 5-to-14-year-old children.
This injury impacts young people and their families physically, financially, socially and psychologically (Whittaker et al 2019, Filbay & Grindem 2019).
Young people have to learn to live with the consequences of this injury for the rest of their lives and can be faced with compromised quality of life, reduced physical activity, increased risk of further injury and potential early onset of osteoarthritis (Zbrojkiewicz et al 2018, Filbay & Grindem 2019, Ardern et al 2018).
Adolescent ACL injuries also lead to a loss of social identity, social isolation, a negative mood state and reduced physical activity (Whittaker et al 2019, Zadro et al 2019).
It is in the key developmental period of adolescence that deep connections with friends and between friendship groups are formed through shared experiences in sport and exercise (Aloha et al 2019).
Shared decision-making is a process where clinician, patient and, in this case, parent jointly participate in making a health decision (Hoffmann et al 2014, Elwyn et al 2012).
A key part of this is discussing the options, their benefits and harms and considering the patient’s preferences, values and situation (Hoffmann et al 2014, Elwyn et al 2012).
Adolescence is a key transition time and parents are critical in advocating for adolescents while still keeping them central to the decision-making process.
There is a paucity of high-quality evidence guiding rehabilitation and decision-making to help adolescents navigate an ACL injury; the literature has been limited by bias and poor methodology (Ekas et al 2019a).
More recently, the 2018 International Olympic Committee consensus statement on the prevention, diagnosis and management of paediatric ACL injuries has added specific guidelines based on expert consensus, although this still covers a wide range of ages (Ardern et al 2018).
In their scoping review, Dietvorst et al (2020) state that there is currently no specific return-to-sport criteria for children and adolescents after ACLR.
Ekas and colleagues have published well-designed prospective studies for children as opposed to adolescents—in adolescents we need to extrapolate from either child or adult data (Ardern et al 2018, Ekas et al 2019a, Ekas et al 2018, Ekas et al 2019b).
Despite these recent contributions, there is still much to be done because varying skeletal maturity makes it difficult to provide guidelines for the different age ranges and stages of development.
Parents and adolescents rely on being given all the information on treatments available, relevant risks and benefits of each treatment and the expected time frames for key milestones, such as return to play.
It is critical that practitioners involved in the care of our most vulnerable population are working to a shared decision-making model and keeping the best interests of the patient foremost (Ardern et al 2018).
Presentation
A 15-year-old female patient (JW) presented for assessment in early July, nine months after an ACLR on her left knee (L-ACLR).
The purpose of the assessment was to determine her suitability for an ACL knee brace to go skiing.
JW is a novice recreational skier and social tennis player who skis 1–2 times per year in Australia for up to three weeks at a time in 5–7-day blocks and trains twice per week for tennis.
JW had an isolated L-ACL rupture in September 2019 while skiing and reports that her injury occurred on take-off when jumping over an obstacle.
She underwent an ACLR using a hamstring graft with a lateral loop in October 2019 and reports having physiotherapy two times per week for 3–4 months following the ACLR.
Approximately two weeks prior to this appointment, JW saw her previous physiotherapist to check her home exercise program and reports that she failed her side-to-side hop test but passed her forward/backward hop test; she was not able to articulate any further what these tests were.
The patient reported that she had been undertaking her home program over the past couple of months on an ad hoc basis at best.
She had commenced tennis training in the past four weeks, which consisted of standing drills from the baseline and at the net, leading with her right (unaffected) leg.
In her most recent surgical review at the seven-month postoperative mark, JW was advised by her surgeon that skiing was possible in July.
JW’s treatment goal was to determine her suitability for an ACL knee brace to go skiing.
JW’s mother called the clinic to book a knee brace fitting.
Following a long discussion, during which I expressed my concern about JW skiing nine months after surgery, she agreed to book an assessment for her daughter.
With a medical history that was otherwise clear and unremarkable, the patient and her mother report JW as being in excellent health and without any growth spurt in the past 12 months.
JW and her mother were very positive about the prognosis and expected a complete recovery and return to full function.
JW lives at home with her parents and younger sister.
On the basis of her history alone, there were significant concerns about JW skiing in two weeks’ time given her age, that it was only nine months since her ACLR and that she described an incomplete rehabilitation program.
An extensive explanation of the International Olympic Committee guidelines of not returning to sport for 12 months after an ACLR was provided, along with an explanation of the increased risk associated with an early return to sport (Ardern et al 2018, Beischer et al 2020).
The risk of injury either to her graft or to her contralateral knee, even 12 months after an ACLR, was also explained (Ardern et al 2018, Beischer et al 2020, Webster & Feller 2016).
The battery of tests, the risks and benefits of the testing and that there was a chance of reinjury were explained.
Verbal consent was obtained from both parties and documented.
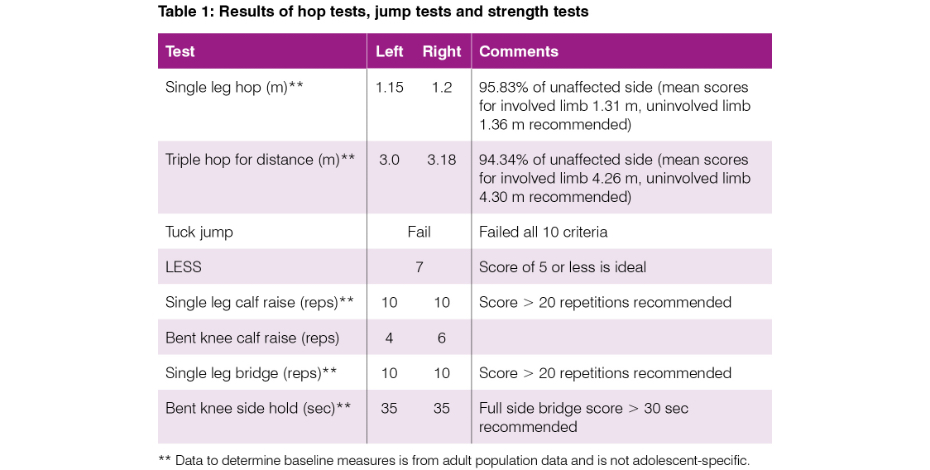
Hop testing, tuck jump test and landing error scoring system (LESS) test were all conducted, along with strength tests as outlined in Table 1.
In addition, the AxIT system (Strength by Numbers, Australia) was used to assess lower limb strength and power via a dual force plate system and push dynamometer.
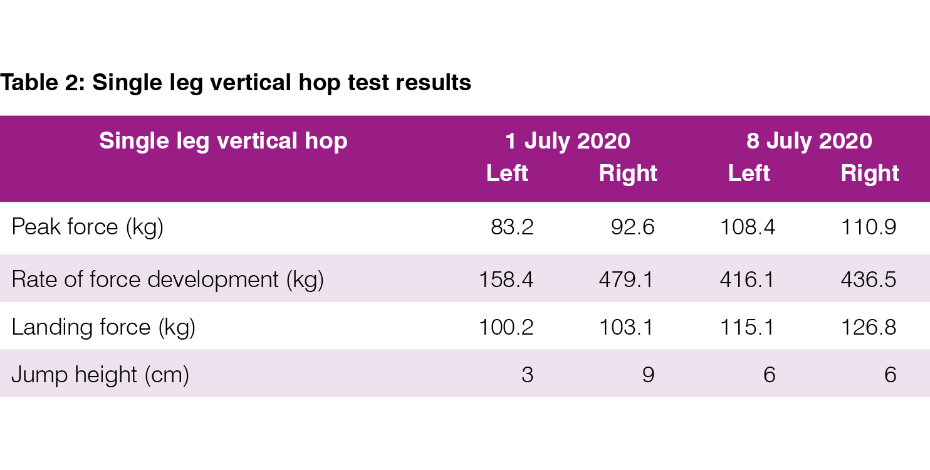
To keep this case study concise, only the single leg vertical hop (SLVH) will be reported as it illustrates individual limb performance in a sport-specific task (Maffiuletti et al 2016).
See Table 1 and Table 2 for an outline of the tests conducted.
In the SLVH, rate of force development (RFD) in particular was a key assessment measure compared to maximal voluntary contraction (MVC)—see Table 2.
RFD appears to be better related to the performance of sport-specific tasks and more sensitive in detecting acute and chronic changes in neuromuscular function (Maffiuletti et al 2016).
During rehabilitation from ACLR, RFD criteria may be a useful adjunct outcome measure in aiding return-to-play decision-making (Buckthorpe &Roi 2018).
The LESS and tuck jump assessment are valid and reliable tools for assessing lower limb neuromuscular control.
They are accessible, inexpensive tools available to clinicians to help determine a patient’s progress in rehabilitation (Fort-Vanmeerhaegheet al 2017, Read et al 2016, Everard et al 2019).
However, like all tests used in this assessment, they are not without their limitations.
The tuck jump assessment has undergone several revisions since its introduction and while it is a useful tool clinically, it is very important to realise that there is no one tool that can help guide decision-making (Smith et al 2017).
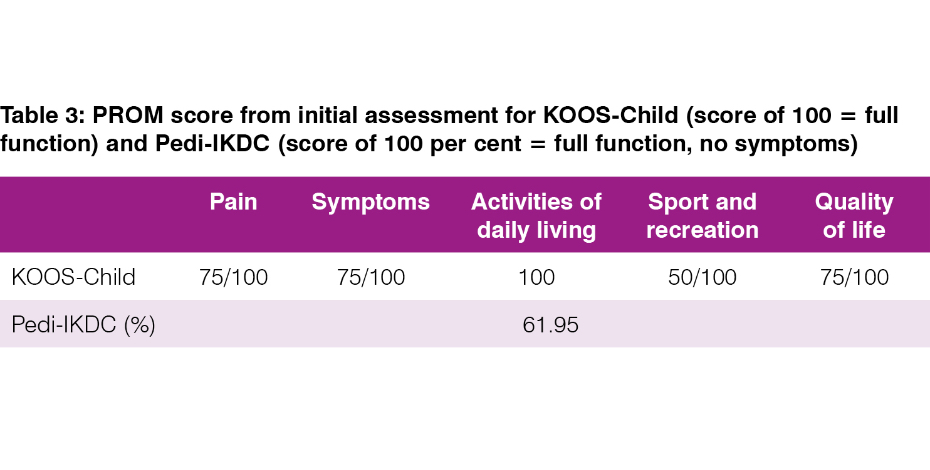
JW also completed the following patient-reported outcome measures (PROMs): Pedi-IKDC and KOOS-Child—see Table 3.
Both of these PROMs have been validated in children and adolescents aged 9–18 years with knee pain, pathology or dysfunction (van der Velden et al 2019).
Adult versions of these PROMs are inappropriate for use due to a lack of comprehensibility (van der Velden et al 2019).
Van der Velden et al (2019) recommend the Pedi-IKDC, as it showed better psychometric properties and is shorter to complete.
Following the physical assessment, there was a long discussion with JW and her mother about her assessment and goal of going skiing in two weeks’ time.
While the results on hop testing were similar for each leg, recent studies have reported that limb symmetry on hopping tests may not correlate with normal knee function, jump or landing mechanics (Wren et al 2018, Kotsifaki et al 2020).
Kotsifaki et al (2020) state that using only hop distance with the healthy or unaffected side as a reference is insufficient to fully assess knee function after an ACLR.
The primary reasons for not recommending a return to skiing at 9.5 months post ACLR were:
- the time frame post reconstruction
- the increased risk of reinjury at this stage of rehabilitation
- JW’s age and sex (Ardern et al 2018, Ekas et al 2019a, Webster & Feller 2016).
In addition to this, the tests conducted demonstrated to JW that there were a number of areas for improvement before she would be physically ready to return to skiing.
All strength measures assessed were inadequate: hop testing, ankle plantar flexors (calf complex) assessed via single leg calf raise and bent knee calf raise, single leg bridge and side hold were all below recommended benchmarks (Gokeler et al 2017, Cooper & Hughes 2018, Herbert-Losier et al 2017).
JW’s previous home exercise program was inadequate to meet the demands of skiing and had not extended beyond double leg squats, clams and calf raises, with little progression of these exercises.
There had not been any exposure to hop and landing exercises for someone who had a goal of skiing in the July school holidays.
JW was given a revised program that addressed the inadequate strength measures recorded at assessment and also included hop and land drills.
Given the closed nature of the tennis training JW described and the psychological and social benefits of being engaged in physical activity with her friends, a decision was made to continue with tennis in this format.
A copy of the 2018 International Olympic Committee consensus statement on prevention, diagnosis and management of paediatric ACL injuries was provided to JW and her mother following the assessment.
JW and her mother were advised that the decision to ski or not was up to them and that they should make a decision based on the recent review with JW’s treating physiotherapist, the assessment conducted and the upcoming review with her surgeon.
The patient was keen for a follow-up and a review appointment in seven days was made.
At her follow-up appointment, JW and her mother reported that they had decided against skiing, that the surgeon was ‘less keen’ on skiing and that they were happy to focus on completing further rehabilitation.
Hop testing was much improved on the force plates in terms of peak force, rate of force development and jump height, with far less side-to-side difference.
This may be attributed to improved motor control and familiarity in completing jumping and landing drills.
JW’s home program was upgraded and the patient was compliant with her exercises.
Discussion
This case demonstrates the value of a sports and exercise physiotherapy-led, objective, criteria-based examination in determining the readiness of an adolescent female to return to sport, particularly in a patient population where there is a paucity of literature to support clinical, chronological or performance criteria to guide return to sport.
In this instance, JW’s primary goal was to purchase a brace for skiing.
It was during the initial phone conversation with JW’s mother that a process of clear questioning was undertaken to determine the need to purchase a brace and facilitate the return to skiing for the patient.
It was quickly apparent that the patient and her mother did not understand what a successful return to sport should entail given the increased risk of returning to sport earlier than 12 months (Ardern et al 2018).
A decision based on whether a knee brace was suitable quickly changed to one based on a return to play.
High-value care is about interventions that provide a large benefit in relation to their cost, do not waste health resources and do no harm (Zadro et al 2019).
This case provides a clear example of high-value care: unnecessary cost (ACL knee brace) was avoided, a return to play (skiing) earlier than recommended by international practice guidelines was delayed, assessment of current capabilities and limitations was conducted and a home-based program was prescribed.
At about one-quarter of the cost of an ACL knee brace, the patient received high-value care.
Strength measures in all tested parameters were inadequate and further increased her risk of potentially either re-rupturing her graft or injuring the contralateral knee.
The ACL Return to Sport after Injury (ACL-RSI) is a tool that could have been used to assess the patient’s psychological readiness to return to sport (McPherson et al 2019a).
A score of less than 77 points in the ACL-RSI indicates that patients under 20 years of age have a higher risk of a second ACL injury and may benefit from psychological counselling before being cleared to return to sport (McPherson et al 2019b).
It is important to note that the ACL-RSI has not been validated in patients under 16 years of age; it is unknown how this affects the validity of using this tool.
On reflection, this could have been administered to provide a comprehensive picture of the patient’s progress in her rehabilitation.
While a return to skiing was not recommended at this time for the reasons previously mentioned, the ACL-RSI would have provided helpful information as part of her rehabilitation and given guidance for future rehabilitation.
One of the key issues in managing ACL injuries in an adolescent population is the lack of high-quality evidence and specific tools and criteria (Dietvorst et al 2020).
Additionally, there was no discussion of ACL graft healing, ligamentisation of the graft or some of the other risk factors associated with return to sport earlier than 12 months following an ACLR (Pouderoux et al 2020, Ho 2018).
I could have discussed these in future appointments.
By following the guidelines and based on the assessment and discussions, JW was happy to delay her return to play.
In doing so, issues with graft healing, ligamentisation, sex and age were avoided.
If the patient and her mother were still looking at an early return to play, another conversation would have been undertaken to unpack the issue further.
This case details the application of recommendations based on the best available practice guidelines to provide high-value care to an adolescent nine months after an ACLR in a sports and exercise physiotherapy-led, objective, criteria-based examination.
Consent was obtained from the patient and her mother to use specific information and details as required for this case study.
>> APA Sports and Exercise Physiotherapist and APA Musculoskeletal Physiotherapist Scott Wilson, MACP, is a Sports and Exercise registrar undertaking Fellowship of the Australian College of Physiotherapists by Clinical Specialisation and is the host of the Young Athlete Podcast.
- References
1. Zbrojkiewicz, D., C. Vertullo, and J.E. Grayson, Increasing rates of anterior cruciate ligament reconstruction in young Australians, 2000-2015. Med J Aust, 2018. 208(8): p. 354-358.
2. Whittaker, J.L., C.D. McKay, and M.E. Batt, Prevention, management and long-term consequences of sport and exercise-related musculoskeletal disorders. Best Pract Res Clin Rheumatol, 2019. 33(1): p. 1-2.
3. Filbay, S.R. and H. Grindem, Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best Practice & Research Clinical Rheumatology, 2019. 33(1): p. 33-47.
4. Ardern, C.L., et al., 2018 International Olympic Committee consensus statement on prevention, diagnosis and management of paediatric anterior cruciate ligament (ACL) injuries. Br J Sports Med, 2018. 52(7): p. 422-438.
5. Zadro, J.R., et al., Choosing Wisely after a sport and exercise-related injury. Best Pract Res Clin Rheumatol, 2019. 33(1): p. 16-32.
6. Aloha, A., L. Krizza, and C. Emma, The friend that got away: an exploration on female adolescent’s friendship dissolution. University of Mindanao International Multidisciplinary Research Journal, 2019. 4(1): p. 34-46.
7. Hoffmann, T.C., et al., Shared decision making: what do clinicians need to know and why should they bother? Med J Aust, 2014. 201(1): p. 35-9.
8. Elwyn, G., et al., Shared decision making: a model for clinical practice. J Gen Intern Med, 2012. 27(10): p. 1361-7.
9. Ekas, G.R., et al., Coping With Anterior Cruciate Ligament Injury From Childhood to Maturation: A Prospective Case Series of 44 Patients With Mean 8 Years' Follow-up. Am J Sports Med, 2019. 47(1): p. 22-30.
10. Ekas, G.R., et al., New meniscal tears after ACL injury: what is the risk? A systematic review protocol. Br J Sports Med, 2018. 52(6): p. 386.
11. Ekas, G.R., et al., Knee Pathology in Young Adults After Pediatric Anterior Cruciate Ligament Injury: A Prospective Case Series of 47 Patients With a Mean 9.5-Year Follow-up. Am J Sports Med, 2019. 47(7): p. 1557-1566.
12. Beischer, S., et al., Young Athletes Who Return to Sport Before 9 Months After Anterior Cruciate Ligament Reconstruction Have a Rate of New Injury 7 Times That of Those Who Delay Return. J Orthop Sports Phys Ther, 2020. 50(2): p. 83-90.
13. Webster, K.E. and J.A. Feller, Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am J Sports Med, 2016. 44(11): p. 2827-2832.
14. Maffiuletti, N.A., et al., Rate of force development: physiological and methodological considerations. Eur J Appl Physiol, 2016. 116(6): p. 1091-116.
15. Buckthorpe, M. and G.S. Roi, The time has come to incorporate a greater focus on rate of force development training in the sports injury rehabilitation process. Muscles, ligaments and tendons journal, 2018. 7(3): p. 435-441.
16. Fort-Vanmeerhaeghe, A., et al., Intra- and Inter-Rater Reliability of the Modified Tuck Jump Assessment. J Sports Sci Med, 2017. 16(1): p. 117-124.
17. Read, P.J., et al., Reliability of the Tuck Jump Injury Risk Screening Assessment in Elite Male Youth Soccer Players. J Strength Cond Res, 2016. 30(6): p. 1510-6.
18. Everard, E., M. Lyons, and A.J. Harrison, Examining the Reliability of the Landing Error Scoring System With Raters Using the Standardized Instructions and Scoring Sheet. J Sport Rehabil, 2019: p. 1-7.
19. Smith, C.A., Chimera, N.J., Lininger, M.R., Warren, M., Modified Tuck Jump Assessment: Reliability and Training of Raters. Journal of Sports Science and Medicine, 2017. 16: p. 440-442.
20. van der Velden, C.A., et al., Pedi-IKDC or KOOS-child: which questionnaire should be used in children with knee disorders? BMC Musculoskelet Disord, 2019. 20(1): p. 240.
21. Wren, T.A.L., et al., Hop Distance Symmetry Does Not Indicate Normal Landing Biomechanics in Adolescent Athletes With Recent Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys Ther, 2018. 48(8): p. 622-629.
22. Kotsifaki, A., et al., Measuring only hop distance during single leg hop testing is insufficient to detect deficits in knee function after ACL reconstruction: a systematic review and meta-analysis. 2020. p. 139-+.
23. Gokeler, A., et al., A critical analysis of limb symmetry indices of hop tests in athletes after anterior cruciate ligament reconstruction: A case control study. Orthop Traumatol Surg Res, 2017. 103(6): p. 947-951.
24. Cooper, R., Hughes, M., The Melbourne ACL Rehab Guide 2.0. 2018. p. 32.
25. Hebert-Losier, K., et al., Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy, 2017. 103(4): p. 446-452.
26. McPherson, A.L., et al., Smaller Change in Psychological Readiness to Return to Sport Is Associated With Second Anterior Cruciate Ligament Injury Among Younger Patients. Am J Sports Med, 2019. 47(5): p. 1209-1215.
27. McPherson, A.L., et al., Psychological Readiness to Return to Sport Is Associated With Second Anterior Cruciate Ligament Injuries. Am J Sports Med, 2019. 47(4): p. 857-862.
28. Dietvorst, M., et al., Limited evidence for return to sport testing after ACL reconstruction in children and adolescents under 16 years: a scoping review. J Exp Orthop, 2020. 7(1): p. 83.
29. Pouderoux, T., B. Muller, and H. Robert, Joint laxity and graft compliance increase during the first year following ACL reconstruction with short hamstring tendon grafts. Knee Surg Sports Traumatol Arthrosc, 2020. 28(6): p. 1979-1988.
30. Ho, B., Risk Factors for Early ACL Reconstruction Failure in Pediatric and Adolescent Patients: A Review of 561 Cases. Journal of pediatric orthopedics, 2018. 38(7): p. 388.
© Copyright 2024 by Australian Physiotherapy Association. All rights reserved.





{kind=link}
{kind=link}
{kind=link}